Parents often ask whether or not their child is walking “normally”. In most cases, their gait (walking pattern) will be normal with no reason for concern. There are a huge variety of toddler gait patterns. What you may consider abnormal may be a ‘typical’ gait pattern for your child's age and/or stage.
Although parents often worry about the following, these are considered normal variations in a child’s gait.
Bow Legs/Knock Knees
Bow legs and knock knees are part of the normal development of children’s legs and will change as they are growing. Vitamin D is essential for keeping bones healthy, find out more on our Vitamin D page.
For more information and advice look at:
When to seek help:
Please contact your local
paediatric physiotherapy advice line if:
- the bow legs or knock knees is only on one side
- it is stopping the child or young person doing normal activities such as walking and running.
 Curly/Crossed Toes
Curly/Crossed Toes
Congenital curly/crossed toes can occur on one or both feet and affect the 3rd, 4th and 5th toes. The toes tend to be flexible and don’t interfere with walking.
Flat Feet
 We know that the majority of children between 1-6 years of age have flat feet. All children before the age of 3, have flat feet, as the arch on the inside of the foot does not begin to develop until after this age. This is part of the normal development of their feet. Over 95% of children grow out of their flat feet and develop a normal arch. The other 5% continue to have flat feet, but only a small number will ever have a problem. Most children with persistent flat feet participate in physical activities, including competitive sports, and experience no pain or other symptoms. It is less important how your foot looks as to how it functions. Most children with painless flexible flat feet do not need any treatment.
We know that the majority of children between 1-6 years of age have flat feet. All children before the age of 3, have flat feet, as the arch on the inside of the foot does not begin to develop until after this age. This is part of the normal development of their feet. Over 95% of children grow out of their flat feet and develop a normal arch. The other 5% continue to have flat feet, but only a small number will ever have a problem. Most children with persistent flat feet participate in physical activities, including competitive sports, and experience no pain or other symptoms. It is less important how your foot looks as to how it functions. Most children with painless flexible flat feet do not need any treatment.
For more information and advice look at:
When to seek help:
Please contact your local
paediatric physiotherapy advice line if:
- your child or young person cannot squat down to pick up a toy with their heels on the floor.
- they are complaining of pain.
Frequent Falls
Falls are part of every baby and toddler’s daily life. Falls help children learn how to get back up, problem solve, strengthen their core muscles, and also work on their balance. One study has found that on average, a group of normally developing one year old children fell 17 times an hour. The number of falls should reduce as children get more practice walking independently. They should be given as much opportunity to do this as possible. Choosing the correct footwear will help provide stability around the ankle, thus helping to reduce falls. If your child continues to fall frequently it can be helpful to get their vision checked to make sure this is not the cause.
When to seek help:
If the falls are new and your child was previously steady on their feet but they are now falling often, please contact a health professional urgently (contact your GP or call 111).
Please contact your local paediatric physiotherapy advice line if:
- the falls are being caused by asymmetry in their walking pattern.
- the frequency of falling is not reducing in line with their overall developmental progress.
- the falls are impacting on or interfering with your child's development.
Intoeing

Some children’s feet turn in when they walk. This is called intoeing or ‘pigeon toe’ and is very common in young children. It is one of the most common normal variants in children and is usually seen in both feet but may be just one. It is normal for toddlers and young children to walk with their feet facing in the way. It is more common than out-toeing. Your child may appear to trip more often but this will get less in time.
 Intoeing is more common in children who 'W' sit. Encourage your child to sit with their legs in a basket, out in front of them or tucked to the side. Intoeing tends to happen on both sides. It usually resolves by 8-10 years of age.
Intoeing is more common in children who 'W' sit. Encourage your child to sit with their legs in a basket, out in front of them or tucked to the side. Intoeing tends to happen on both sides. It usually resolves by 8-10 years of age.
For more information and advice look at:
When to seek help:
Toe Walking
 Toe walking is walking on tip toes or when the heel doesn't touch the ground. It can happen some, most or all of the time. Toe walking is a normal part of development and lots of children grow out of this. In some cases toe walking can continue into adulthood. Toe walking can sometimes be due to other conditions like cerebral palsy, muscular dystrophy or neurodevelopmental differences like autism.
Toe walking is walking on tip toes or when the heel doesn't touch the ground. It can happen some, most or all of the time. Toe walking is a normal part of development and lots of children grow out of this. In some cases toe walking can continue into adulthood. Toe walking can sometimes be due to other conditions like cerebral palsy, muscular dystrophy or neurodevelopmental differences like autism.
For more information and advice look at:
When to seek help:
Please contact your local
paediatric physiotherapy advice line if:
- toe walking is only on one side
- your child or young person has suddenly started toe walking
- they are unable to put their heels flat on the floor when standing
- their legs feel stiff
- they have pain or discomfort in their calves.
 KIDS for Families
KIDS for Families
 When your baby is born, labour can cause their head to become misshapen. This is normal and corrects within the first few weeks after birth.
When your baby is born, labour can cause their head to become misshapen. This is normal and corrects within the first few weeks after birth. Tummy time helps build muscles that your baby needs for activities like sitting and crawling. It also helps your baby develop a more rounded head shape.
Tummy time helps build muscles that your baby needs for activities like sitting and crawling. It also helps your baby develop a more rounded head shape. Some children W-sit. This is when they sit on the ground, with their bottom, knees, and feet all touching the ground. Their feet will be resting outside their knees. When looking at the seated position from above, it resembles the letter ‘W’.
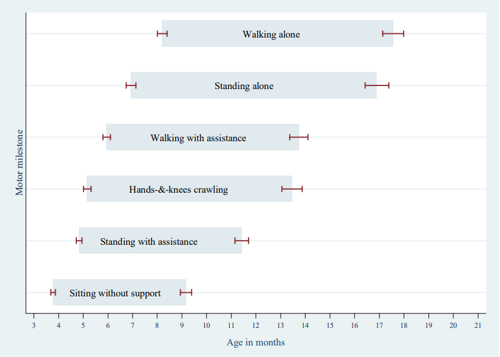
Some children W-sit. This is when they sit on the ground, with their bottom, knees, and feet all touching the ground. Their feet will be resting outside their knees. When looking at the seated position from above, it resembles the letter ‘W’. Most children begin to crawl from between 5 to 13.5 months. Some children don’t crawl up on their hands and knees. Some may:
Most children begin to crawl from between 5 to 13.5 months. Some children don’t crawl up on their hands and knees. Some may: At around 6 months, most babies may stand when held and begin to bounce. They can do this as their core, pelvis and legs muscles strengthen. Many babies will begin pulling up to stand about 9 months and most will stand at the sofa or with hands held by 12 months. Some babies dislike standing especially if they enjoy bottom shuffling. Some babies don't like the feel of the flooring on their feet e.g carpet, sand, lino, grass, wood, stone.
At around 6 months, most babies may stand when held and begin to bounce. They can do this as their core, pelvis and legs muscles strengthen. Many babies will begin pulling up to stand about 9 months and most will stand at the sofa or with hands held by 12 months. Some babies dislike standing especially if they enjoy bottom shuffling. Some babies don't like the feel of the flooring on their feet e.g carpet, sand, lino, grass, wood, stone.






